
“You Have to See People and Listen to Them”: Erin Williams on WHAT’S WRONG
Erin William’s graphic narrative Commute hit me hard. In the book, Williams unpacks memories of shame, addiction and recovery, and sexual assault through the analysis of the male gaze on a day’s commute to and from work. It’s brutal, vulnerable, and universal in its story of womanhood in America. And as someone who manages chronic pain, when I learned that Williams was writing a book about chronic pain, I was intrigued. I jumped at the chance to interview her.
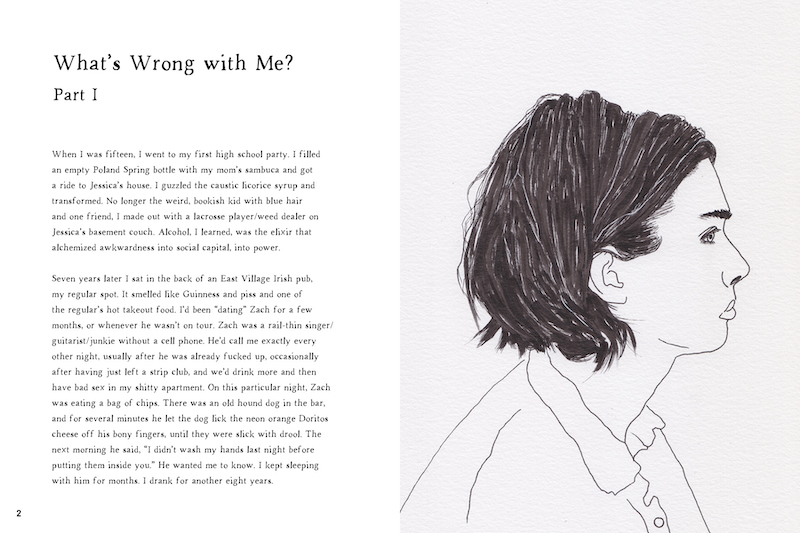
In her newest release, What’s Wrong: Personal Histories of Chronic Pain and Bad Medicine, Williams profiles four individual’s stories of chronic pain and illnesses including cancer, endometriosis, alcoholism, depression, and PTSD, as well as her own journey. The American medical system does not see or believe these people. It fails them.
Williams witnesses their stories. She documents these stories, offering context rooted in each individual’s history, their place in society, and access in the American medical system. Williams spoke with me about her process in creating these portraits and the intersection of pain and parenthood, amongst other topics. – Cara Gormally

Cara Gormally: Why do you think this is so important to tell these stories—to talk about pain?
Erin Williams: I wanted to offer up something that felt vulnerable, authentic, and experienced. I wanted to engage with pain and suffering on a different level, from a place that’s not about generating empathy. Having bodily sensations that are unruly, unable to be tamed by the rational mind is hard to integrate, especially when your body is a sight of trauma. And nobody has the language to talk about these things in a way that’s meaningful, productive or helpful.
There are 20 million people living in this country who have chronic pain. Our American health care system is very good at acute pain. But for chronic pain there’s very little hope and very few good treatments. And a lot of it is very difficult to afford. So what do we do? We turn to plants, art, community. Sharing stories is certainly part of that. Here are 4 of those 20 million people and this is what it’s like for them.
CG: To me, reading What’s Wrong gave me this opportunity to witness people’s lives. To see how pain and trauma shape somebody’s life—and can take over one’s life, like tentacles.
EW: Every bad health outcome in this country comes down to the individual and individual decisions. We talk about one bad doctor: We can look at someone like Dee. We look at her history. And we can say “well, this doctor made a bad call–it wasn’t the right decision to give her a hysterectomy,” but really you have to go back and understand the bigger context. A doctor and a patient are in a room for a 15 minute visit. But alongside the doctor and patient in that room–centuries of things that have happened that inform those 15 minutes where critical treatment decisions are made. In making this book, that was a huge part for me–to show how these decisions are made in these bigger contexts over the course of someone’s life from early childhood trauma to chronic pain in adulthood. I wanted to show how these medical decisions made by their clinicians stack up over time. I wanted to show how time and structural oppression in health care informs each of these clinic visits. When Dee, as a Black woman, is prescribed Depo Provera as a form of birth control, why was she given that? Why was I, as a white woman, given something else? That birth control prescription irreparably changed the course of her life. I wanted to show the reader that context. I largely let the people whose stories are in this book tell their stories in their own words. To support their words, I used medical data and statistics and historical context. And the art offers relief.

CG: Tell me about the art. I noticed there were so many different styles of art in the book. To me, the art offered room to breathe, to pause, to take in the stories.
EW: Visually, the book is very different than Commute. I spent years trying to figure out what the visual language for this book would be, what made the most sense. Early versions of it looked much more like Commute. But I wanted each person in the book to have their own color story. From there, I went to this more cartoony style in color. Before that I had line drawings. But it didn’t feel vulnerable enough. So I started drawing pencil on paper and watercoloring and messing around with ink. Having my hands on a physical piece of paper made a lot of sense for this book. The process felt authentic and visceral. I combined digital pieces and hand-rendered pieces.
I had a mentor, Dr. Sacks, who is quoted in the book. He says that “science has nothing to say about what it is like to actually be an individual thing.” But that art does. John Dewey wrote that when artistic objects are separated from the conditions of origin, a wall is built around them that renders almost opaque their general significance. I think that is what happens with Western medicine. We separate the conditions of origin from the symptoms and we try to treat them. We’re not treating the whole person. What Dr. Sacks says is that art can tell us something about what it’s like to be a person.
I had a lot of conversations with the people whose stories are in this book about how I could visually represent them. This is why you see Rain often appearing as a ghost or Alex as limbs, in pieces, which is what dissociation can feel like after sexual trauma. It was really important to me to figure out a way to capture their perspectives through the art. And as a white woman with a lot of privilege, it was important to me to not spectacularize somebody else’s pain. I really wanted to figure out how to represent their pain abstractly. I was not going to show a picture of a body being cut open or actual violence to a person’s body. I wanted the art to communicate the pain, with care.

CG: Later in What’s Wrong, you write “each of us needed to see each other and to be seen.” I don’t want to use the word “healing” because I feel like it’s not like that—it’s an impossibility in some way—chronic pain is ongoing. But I’m wondering about the power of seeing each other and being seen. That seems deeply nourishing. Tell me more about that.
EW: I also hate the word “healing.” “Yeah, all done. We’re good now.” It’s like in Goodwill Hunting when Matt Damon walks into therapy for the first time and says “all right, let the healing begin!” It’s not like that.
Yet one of the most mind blowing things about having done this work is if you called any of the people who appear in this book, they would say to you that this process was very healing for them. That really blew my mind. When I finish a book that’s about myself, it never feels healing for me. I’m still recovering from Commute.
This book was a lot of difficult very personal conversations over the course of years. I was very intentional about how I wanted to approach these conversations. I wanted to make sure that I had the ability to do their stories justice.
My relationships with the people whose stories are in the book are the most amazing gift.
In my initial conversations with them, I said “This is your story. I will send you every draft. Every version. Every piece of art, you can say no to anything you want. You can change anything you want. This is yours, you’re in control.” And I did that. Every couple of months I sent them work and asked: “Are you okay with this? Are you okay with this?” Because sometimes in an interview people tell you things and then later they don’t want to reveal that.
With a journalistic book, you get people’s medical records to verify their stories–to confirm that what Dee says is true about her own experience based on what the doctor said. I wasn’t gonna do that. I’m going to believe what you tell me about your own lived experience. I’m going to trust you. But to me, this is not a purely journalistic project. It is an exercise in saying, “Look at what happened. Here’s the context. And I believe that this happened to you and I believe that you feel this way and I’m going to represent it the way that you’ve lived it.” It’s a really powerful thing. I think that that is the heart of feeling seen and being seen.
There’s not enough of that in medicine. You’re telling me that this part of your body hurts, but it’s not on the scan, your blood counts are normal, so we don’t believe people when they say they’re in pain if doctors can’t see it? I wanted to just believe—I wanted to believe what people tell me when they say they’re suffering—to just believe them. And to tell them “I’m really sorry this happened to you and I want to help you tell your story.”

CG: What’s your hope with this book? I can imagine that medical practitioners need to read this. But beyond that—what is your hope for it?
EW: I have many dreams. One of my dreams is that I talk to medical students. I’ve worked in hospitals. I’ve worked in clinical research. I speak that language a bit. I know so many wonderful, intelligent, smart, warm, well-intentioned doctors. Almost all of them are like that, right? But the problem is structural. When you have 15 minute appointments, when you’re seeing patients, say, in an underserved community where everybody has chronic conditions, like asthma from pollution or type 2 diabetes because they’re living in food deserts–you get 10 minutes with this person and you can’t fix that. So there’s a feeling of hopelessness.
I’m not here to instruct anyone how to feel or to say “here’s an empathy exercise for you.” I think seeing and listening are undervalued skills. Believing people when they tell you what they’re going through or what they’ve been through. Also, understanding while our culture believes that medicine is objective, it’s not. There is no such thing as medical objectivity. You have to see people and you have to listen to them. That’s your first source of data. That’s the most important source of data. You’re treating a human being. You’re not treating symptoms. These structural problems are embedded in the practice of medicine. There are things that would vastly improve health outcomes for many people. But I also feel kind of pessimistic about it because it’s so structural. Maybe we just need a revolution to just start over. To burn it down. But in the meantime, I do believe in progress and in art.
CG: I’m curious about the intersection of pain and parenthood in your book. At one point you say, “I’m mothering both of us, teaching both of us the possibility of a new kind of ease, surrender.” Why is this intersection so critical to share?
EW: Becoming a mother is the most painful thing I’ve ever done. It’s certainly the hardest thing that I’ve ever done. I’ll just speak for myself. I have a lot of early life trauma. I have survived it by dissociating from my body. So, I’m one of those people who’s terrible in therapy because I just want to intellectualize everything, like “now I understand.” And I do understand. I don’t feel things very well. I don’t like feelings. Feelings are disruptive, annoying, big, messy. They’re not productive at all and I don’t really want to feel them anywhere in my body. I would prefer to just be a brain. It’s not my choice that I’d have feelings.
Then I got pregnant. All of a sudden there’s a hostile alien takeover—I have no control over my body. And then I had this labor and delivery which were also totally out of control. You can’t intellectualize your way out of that one. You know, it is a physical process. And then you have this newborn. Right? And they’re needy. They need things from you—every 2 hours at a minimum. So it’s a very physically and emotionally demanding process bringing new life into this world. Labor, delivery, and pregnancy can be particularly triggering for people who’ve been sexually assaulted, because of that loss of control. I struggled with breastfeeding and then I had postpartum depression. I didn’t think that I would survive it. I did. Later, when my daughter was 3 or 4, I had another episode of severe depression. Having these experiences, it’s all full of pain and suffering.
Becoming a mother feels like your body is ripped in half and then you emerge as this new being who has a baby. It’s a very alienating process. You’re relearning who you are. I really struggled when my daughter was young. I didn’t know how to emotionally support her. I didn’t know how to stay with her when she was having these giant feelings. I just wanted to leave. I really just wanted to say “You are not being rational right now. Let’s talk about this when you are being normal.” But she’s 3. I had to learn to sit with a lot of discomfort. Against all of my instincts I had to sit in a lot of pain and discomfort. I had to rewire my brain. My dear friend said to me “In learning to parent her, you’re also reparenting yourself.” Now there are parts of me that know how to sit through discomfort. Parts that know I don’t have to narrativize and intellectualize every feeling.
I know that on good days. Even if my body is uncomfortable or painful, it’s still a safe place.
My body can be a safe place for me and I can be a safe place for her. But it’s a years-long process, to untie all of the knots that have been holding me together for so many decades. Becoming a mother has been the most profound thing that I’ve ever experienced. With the biggest steepest hardest learning curve. But the most rewarding, certainly.

Pages excerpted from WHAT’S WRONG: Personal Histories of Chronic Pain and Bad Medicine by Erin Williams. Copyright © 2024 by Erin Williams. Published and reprinted by permission of Abrams ComicArts, a division of ABRAMS. All rights reserved.
About the Author
Cara Gormally is a biology professor who draws comics to make science relevant to everyday life. Their autobiographical science story comics have appeared on Medium’s Spiralbound and at Popula, among other places. See more on Instagram and at caragormally.com. Their debut book, REBOOT, will be published by Street Noise Books in 2025.
Related Posts

Drama in the Mommune: Domenica Ruta Talks to Jade Sanchez-Ventura About Her Radical Summer Read →

Hard-Earned Patience: An Interview with Hannah Grieco →
Come With Us: An Excerpt from LIVING, TOGETHER →
